
Background
Traumatic brain injury (TBI) is the leading cause of cognitive and behavioral deficits worldwide with ~50 million occurrences that cost $400 billion annually. While neuroimaging is used to diagnose moderate-to-severe TBI, 90% of TBIs are mild-TBI/concussions (C) that are associated with minor /no symptoms and microscopic damage with no observable pathology on neuroimages. Therefore, the diagnosis of concussion remains difficult and sometime inconclusive, relying on clinical symptoms, rather than biomarker measures. Equally important are the asymptomatic sub-concussive (SC) head exposures that when left undiagnosed put the subjects at higher risk of repeated exposures and subsequent injury, resulting in cognitive declines and initiation of chronic neurodegenerative disease. TBI cause cellular disruptions in the brain which initiate a variety of neuroinflammations and metabolomic dysregulations which have shown to be reflected in variety of biofluids. While invasive CSF and minimally invasive blood biomarkers are valuable in TBI diagnosis, they are less practical in routine assessment of repeated asymptomatic C/SC exposures in sports/military settings where C/SC rates are high. Exhaled breath (EB), which expresses various metabolites, proteins, and cytokines, can be a non-invasive alternative approach. Although EB has recently joined blood as a primary biofluid for diagnostic of different diseases like cancer, Alzheimer’s, and Parkinson Disease, it has not been explored for diagnosis of TBI. Given the recent success in EB biomarker for brain-related disease, we hypothesize that brain cellular disruptions/damages due to TBI will be reflected in EB.
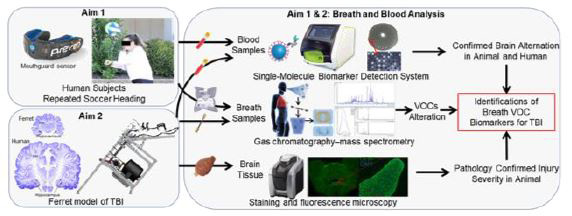
Figure 1. Experimental overview of TBI investigation.
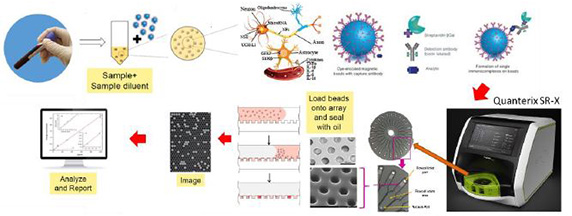
Figure 2. Blood biomarker analysis overview.
Approach
- Aim 1: Identify exhaled breath volatile organic compounds (EB VOC) alterations following sport-related repeated sub-concussion (RSC). Blood and EB-VOC biomarkers will be measured prior to and at 1-hour (immediately), 1-day (acutely) following head exposures.
- Aim 2: Discover EB biomarkers due to mild-TBI in animal model. TBI group goes under repeated closed head impacts and biomarkers in blood and VOCs in EB will be measured prior and at 1-hour, 1-day post-TBI. The EB VOC biomarkers will be correlated with blood biomarkers and neuropathology outcomes.
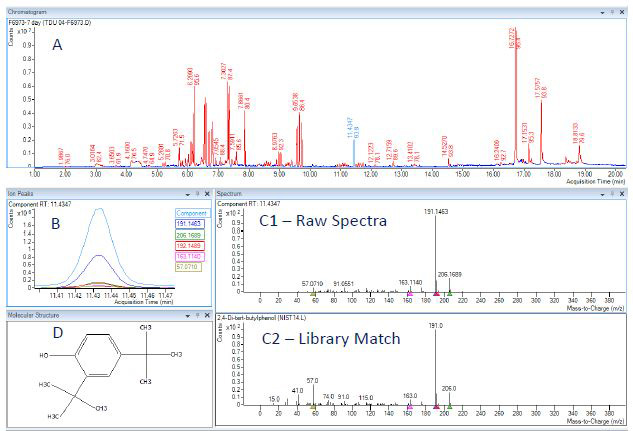
Figure 3. Experimental data for breath-based VOC analysis of TBI subject. Preliminary data for captured breath and analytical analysis via gas chromatography and mass spectrometry (GCMS) at SwRI. Insert (A) is the chromatogram; signal as a function of time, representing the separated compounds contained in the breath sample. Insert (B) is the independent signal for a selected compound. Insert (C) is the structure of the selected compound. Insert (D1) is the mass spectra; signal as a function of m/z ratio and Insert (D2) is the library match for the selected compound.
Accomplishments
- Aim 1: Elevation of TBI blood biomarkers following human RHI confirming brain alteration. Blood samples (16 subjects, 4 time points) were assessed for well-studied TBI-related biomarkers, GFAP (glial fibrillary acidic protein) and NFL (neurofilament light chain) using a single molecule array (Simoa, Quanterix) system to evaluate potential brain disruption following RHI in humans.
- Aim 2: Elevation of TBI blood biomarkers following repeated TBI in animal model. Blood samples (6 animals, 6 time points) were assessed for well-studied TBI-related biomarkers, GFAP and NFL to evaluate TBI.
- Developed an AI model for assessing astrocyte reactivity following TBI.
- Designed a novel breath collection system for reproducible and quantitative analysis.